Renal Stone (NEPHROLITHIASIS) & HOMOEPATHY- By Dr A.K Dwivedi


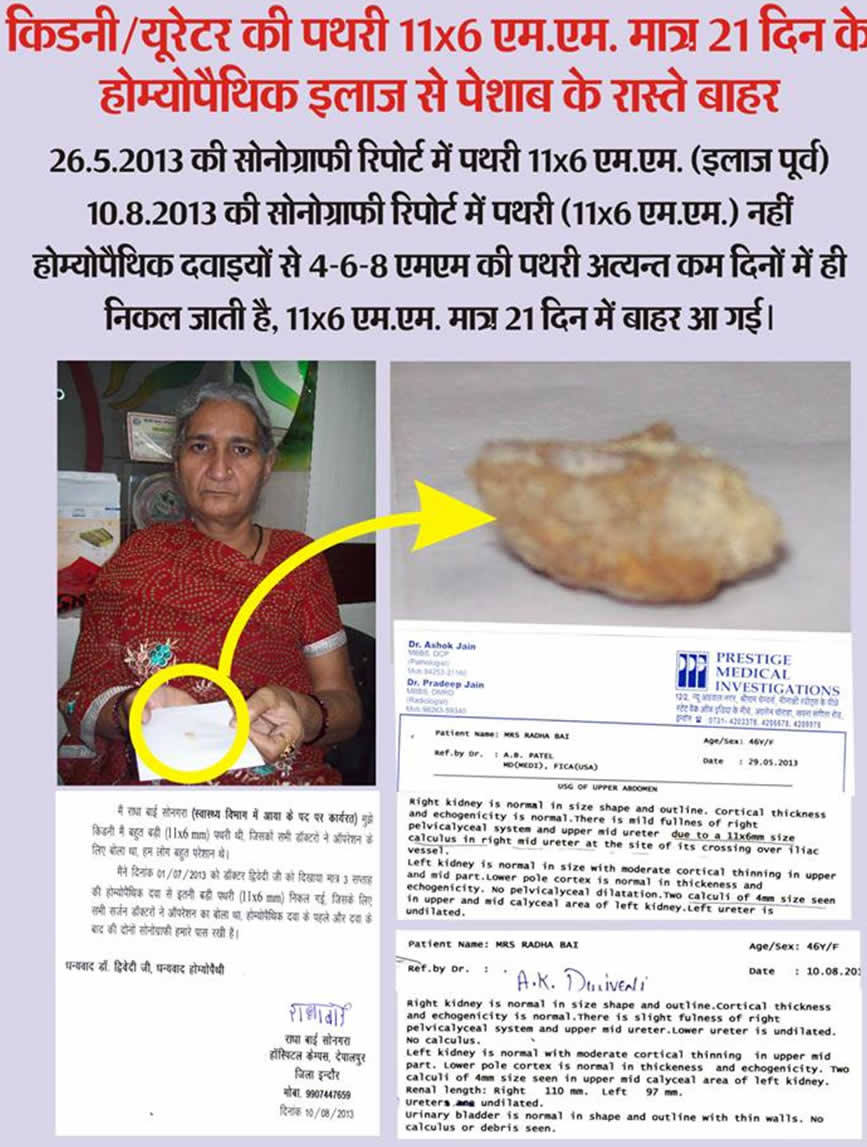
A female patients aged 46 yr. attended my clinic 1st time on 1-7-2013 with sonography report showing multiple renal stone largest being 11 × 6 mm.
After examining the patients I explained to the patient & their relatives that this larger stone can’t pass from urethra with homoeopathic medicines but smaller will be passed very easily. I had given her Homeopathic medicine for 7 days & suggested then if pain or problems increase please admit her any hospital under super vision of some doctors.
After 7 days patients again come to my clinic having no complaints. I have again repeated the same medicine for 15 days’ & told her to come after that sonography report to be done by the same center.
Patients again come to my clinic after 1 month having no complaints with sonography report & stone of 11 × 6 mm in their hands, sonography reports confirm the same.
Renal stone or calculus or Lithiasis is one of the most common diseases of the urinary tract.
- Occurs more frequently in men than in women and in whites than in blacks.
- Rare in children. It shows a familial predisposition.
- World wide in distribution and common in U.S, SOUTH AFRICA, INDIA , SOUTH EAST ASIA
Urinary calculus is a stone - like body composed of urinary salts bound together by a colloid matrix of organic materials.
It consists of a nucleus around which concentric layers of urinary salts are deposited..
ETIOLOGY
HYPEREXCRETION OF RELATIVELY INSOLUBLE URINARY CONSTITUENTS –
1. Oxalate – Though oxalate is the major component of 70% of all renal stones, yet hyperoxaluria as a cause of formation of such stone is relatively rare. Cabbage, rhubarb, spinach, tomatoes, black tea and cocoa contain large amount of oxalate. Ingestion of excessive amounts of ascorbic acid and orange juice also increase urinary oxalate excretion.
2. Calcium - On regular diets normal urinary excretion of calcium ranges between 200 mg to 300 mg per day. The major calcium in foods are in milk and cheese. Milk and dietary protein also cause increased absorption of calcium from the gut.
3. Uric acid - Many patients with gout form uric acid calculi particularly when under treatment. If the urine is made alkaline and dilute while treating this disease chance of uric acid stone formation is less.
4. Cystine – Cystinuria is an herditary disease which is more common in infants and children. Only a small percentage of patients with Cystinuria form stones.
5. Drug induced stones – In rare cases, the long term use of magnesium trisilicate in the treatment of peptic ulcer has produced radio opaque silicon stones.
LOCATION OF STONES IN KIDNEY

Types of renal calculi
Primary Stones : Are those which appear in apparently healthy urinary tract without any antecedent inflammation. These stones are usually formed in acid urine. Usually consist of calcium oxalate uric acid, urates, Cystine, xanthine or calcium carbonate.
Secondary Stones : Are usually formed as the result of inflammation. The urine is usually alkaline as urea splitting organism are most often the causative organisms. Secondary stones are mostly composed of calcium Ammonium-magnesium phosphate (the so-called triple phosphates).
EFFECTS OF STONE
The size and position of the stone usually govern the development of secondary pathologic changes in the urinary trace.
A. SAME KIDNEY –
- Obstruction
- Infection
B. OPPOSITE KIDNEY
- Compensatory hypertrophy
- Stone formation may be bilateral
- Infection
- Calculus anuria
CLINICAL FEATURES
Symptoms - Symptom wise cases can be divided into 4 groups :-
1. Quiescent calculus – A few stones, particularly the phosphate stones, may lie dormant for quite a long period. These stone are also discovered due to symptoms of Urinary Infection
2. Pain - Plain is the leading symptom of renal calculus in majority of cases (80%). Three types of pain.
a) Fixed renal pain
b) Ureteric colic
c) Referred pain
3. Hydronephrosis
4. Occasionally haematuria is the leading and only symptom
PHYSICAL SIGNS
In majority of cases characteristic physical signs are not present. The signs which may be present and should be looked for are : 
(i)Tenderness
(ii)Muscle rigidity over the kidney may be found in a few cases.
(iii)Swelling - When there is Hydronephrosis or pyonephrosis associated with renal calculus, a swelling may be felt in the flank.
The characteristic of a renal swelling are :-
(a) Oval or reniform in shape
(b) Swelling is almost fixed and cannot be moved.
(c) A kidney lump is ballot able.

SPECIAL INVESTIGATIONS
Blood examination – Hardly reveals any specific abnormality, increased white blood cell associated with infection. Anemia may be found, blood urea, creatinine.
2. Urinalysis –
(i) Physical examination Show smoky urine due to slight haematuria or pale scent due to presence of pus.
(ii) Chemical examination Show presence of protein due to haematuria and blood in the urine. If pH of the urine is higher than 7.6, presence of urea-splitting organism is assured.
(iii) Microscopic examination of urine Show R.B.C. pus cells and casts. Different crystals may be seen in the sediment to give a clue as to the type of stone present. Uric acid of glacial acetic acid, which lowers the urinary pH to about 4.
(iv) Bacteriological examination of urine Highly important including culture and sensitivity tests.
(v) Renal function tests Always be performed in calculus cases. The PSP may be normal even in presence of bilateral stag horn calculi.
3. Radiography
A) STRAIGHT X-RAY - Before taking straight X-ray for KUB region (both kidneys, ureters and bladder), the bowels must be made empty by giving laxative.
B) Excretory Urogram
4. Ultrasonography –
Helpful to distinguish between opaque and non-opaque stones. It is also of value in locating the stones for treatment with extra corporeal shock wave therapy.
5. Computed topography – Particularly helpful in the diagnosis of non-opaque stones.
6. Renal Scan
7. Instrumental examination :- Cystoscopy
8. Examination of the stone
C O N S E R V A T I V E M E A S U R E S
Not all patients with renal stones require surgery.
(i) When the stones are sufficiently small, these can be naturally eliminated and expectant policy is best adopted in these cases.
(ii) In the elderly, poor risk patients a curalliform stone is best left alone unless it causes significant symptoms.
(iii) Chemical dissolution of renal stones requires indwelling urethral catheters for constant through and through irrigation with Renacidin or with G solution. Sometimes stone fragments occlude the ureteral catheters and cause acute obstruction.
With the advent of percutneous Extra corporeal shock wave Lithotripsy (ESWL), this method has mostly become obsolete.
Homeopathic Medicine – Apis-mel, hydrangea, berberis-vulgaris, lycopodium, dooscoria, urtica-urens, benzoic-acid,cantharis, thalaspi etc.
REFRENCES
1.HARRISON,S
INTERNAL MEDICINE, 16th Edition
Page no.1710 Nephrolithiasis
2. DAVIDSON’S
PRINCIPLE & PRACTICE OF MEDICINE, 19th Edition
Page no.632 Urinary Tract Calculi and Nephrocalcinosis
3. BAILY & LOVE
SHORT PRACTICE OF SURGERY 24th Edition
Page no.1315 Renal Calculi
4. JAMES TYLER KENT
LECTURES ON MATERIA MEDICA,Reprint Edition 2000
B.Jain Publisher (P) LTD
5. SAMUEL LILIENTHAL
HOMOEOPATHIC THERAPEUTICS 19th Impression 2010
B.Jain Publisher (P) LTD
Page no.110 Calculi Renales
6. INTERNET




Home | Set as homepage | Add to favorites | Rss / Atom
Powered by Scorpio CMS
Best Viewed on any Device from Smartphones to Desktop.